

“A civilization that proves incapable of solving the problems that it creates is a decadent civilization.”
Aimé Césaire wrote this in his critique of colonialism. Close examination of the legacy of colonialism helps explain the disparate impact of the current healthcare crisis based on race and class. The sick and dying in the US are disproportionately the poor, the black, and the brown. Does anyone really care or is this just our form of domestic incapability of solving the problems that we create in our system?
Who is harvesting our food? Who delivers groceries and prescriptions to the doorsteps of those with a credit card and the internet? Who launders hospital and medical garments? Who provides care in nursing homes? Who rides the subway or the bus to and from work? Who today would argue that these services are not of central importance to our society? But do we act as if the people who provide these services are central?
A service economy has workers. When there is a pandemic killing and incapacitating these central workers, do we callously discard them like so much damaged goods and bring in others? Rationalizing that they were on their last legs anyway as if we knew them. Or worse, do we shake our heads in sadness but do little to address the systemic weaknesses that are revealed by the pandemic?
Do we provide healthcare for these workers? If not, then are these workers just considered expendable humans? Whether their deaths are a thousand, a hundred thousand, or a million, are we really not to consider them our concern? Do we continue our smug indifference to the outsider from our comfortable suburban shelter in place? Like a king’s court packing up and going to the country during a plague, do we passively wait out the disaster that has become the lives of these workers?
We note that corporations that pay low wages have encouraged their workers to apply for food stamps, privatizing profits and socializing the costs of feeding their employees.
What about healthcare? Should we offer an equivalent “healthcare” stamp to all those who need it? Unless one counts emergency room visits as healthcare—in extremis healthcare differing significantly from the concierge service provided with a premium coverage—we offer nothing to these most vulnerable workers working to save our lives but not their own.
When we watch the paucity of testing, the scramble at the local, state and federal level to find PPE and equipment to address the sick and dying, the price-gouging in distribution, the lack of either price or distribution discipline by persons seeking to make a quick buck with little risk, do we see a market acting efficiently? And this scramble is going on worldwide in a setting where the supply is difficult to increase while demand for healthcare explodes.
It is obvious that there is NO market at work.
Rather we merely have sellers doing price arbitrage between countries, between the federal government, one state or another, one hospital or another, one dying patient and another. This situation is a most horrible example of a worldwide as well as domestic market failure.
To think the market can provide a solution for healthcare for these central vulnerable workers is to place ideology over reality. The market is not working and will not work for the vulnerable here or the vulnerable around the world without disciplined intervention by central governments and coordination to provide the public good that is healthcare.
The true poverty in America is in our souls and our lack of willingness as a nation to do enough about this systemic failure.
We can do better if we can raise our expectations as to what government can and should do. For in these circumstances, like sometimes in the law, the market is an ass. And if we are too enamored of the market, we are decadent accomplices in atrocities that harken back to colonialism’s indifference to human life. We need to protect the human right to health and well-being as it is certain that the market fails us all.
We have little problem with regulatory intervention to correct market failure in the form of antitrust laws—and, in case of declared emergencies, we have scattered prohibitions against price gouging. We even protect natural resources from market forces with our nation’s parks. Examples of our correcting for market failures abound. There is no justification for lack of corrective action here unless the shortcomings in our healthcare delivery system are necessary byproducts of a decadent society clinging to aspects of its colonial past.
The rush to re-open the economy is a rush of lemmings to the sea.
As of April 16, 2020, the federal government has proposed a three-phase Opening Up America Again plan. The preconditions for entering the phases (gating criteria) announced are:
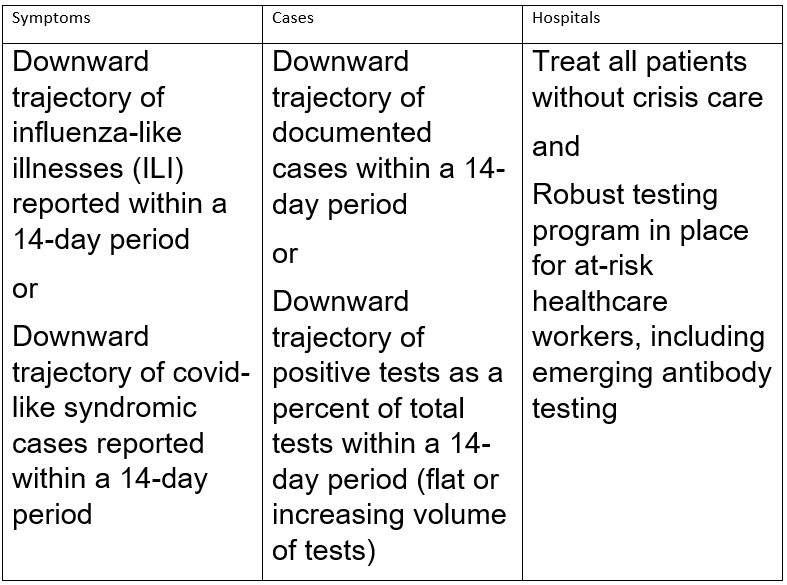
Symptoms: under these guidelines there is an alternative given for gating between Influenza-Like Illnesses (ILI) and COVID-Like Syndromic Cases (CLSC). The actual datasets on the CDC website make a distinction between visits to the emergency department for ILI and COVID-Like Illnesses (CLI). As such, the obvious question is what relevance does a decrease in ILI visits have to the spread of CLI? In addition, the requirement refers to a 14-day downward trajectory in both cases. The definition of an appropriate downward trajectory for the 14-day period is not provided. No doubt we will be assured of some forthcoming “guidance” on the nature of such a downward trajectory, but that may not be enough. It is not clear how a downward trajectory in ILI would have any meaning for CLI (see graph below). The way the criteria are set one could imagine a downward trajectory for ILI and a flat or increasing trajectory for CLI and a state might be able to argue it has complied with the symptom definition. Moreover, the curious inclusion of the word “syndromic” in the CLSC (and not CLI) definition in the guidance—a term that is not used at the level of the datasets raises a question as to whether a definitional sleight-of-hand is being employed with respect to what is the universe of CLI cases as opposed to CLSC cases. So by redefining the word syndromic one can give the impression of declining while in the community as a whole the actual number of CLI cases is stable or increasing.

Cases: the insertion of the term “documented” before “cases” raises a question as to how a case becomes documented. The word “documented” either modifies “cases” or it is redundant. We do not doubt that the word “documented” has significance, but its definition is unavailable. The logical impact of that restriction, however, will most likely be to reduce the number of cases or raise criteria for documentation, which will limit what is considered a case. So rather than a capacious vision of cases, this language suggests a more restrictive vision of cases.
Turning to tests, the downward trajectory of positive tests as a percent of total tests presents a numerator/denominator interplay. If one reduces the number of tests, one by definition reduces the number of positive tests found. If one is not testing much now and one continues to test at that rate then one can maintain the positive tests at a flat level. Moreover, if one is selective in where one does the tests in the 14-day period, it is likely that one can influence the results by choosing where and whom to test. Put another way, both of these criteria—much like the symptoms criteria—seem eminently malleable.
Hospitals: treating all patients without crisis care in a situation where an estimated 20 percent of persons infected are hospitalized and 5 percent of all persons infected go to the ICU, raises the question of what is meant by “crisis care.” Again, this may have a distinct definition but the language is unclear. Turning to robust testing, that testing set up is only for at-risk healthcare workers (meaning that healthcare workers can be divided into at-risk and not-at-risk according to some criteria). Who is included in the definition of at-risk healthcare workers is a mystery. Moreover, this kind of robust testing program is not foreseen for the population of a given state, but only for the healthcare workers. Contrast these gating criteria with the World Health Organization guidelines which are more categoric.
Any step to ease restrictions must ensure:
1. That evidence shows COVID-19 transmission is controlled.
Given the significant wiggle room in the federal government’s gating criteria, it is hard to see that compliance with those criteria will provide evidence that COVID-19 transmission is controlled at all.
2. That public health and health system capacities, including hospitals, are in place to identify, isolate, test, and trace and quarantine contacts.
Again, the gating criteria say nothing about identifying, isolating, tracing, and quarantining and only marginally discuss testing in two forms that are easily manipulated. In addition, the capacity issue on each of these crucial tasks is omitted from the discussion when we know that testing and the related material and personnel needed to do this properly are lacking across the US. The proposed federal guidelines do not speak to availability of resources, such as gloves, masks, ventilators and other essential equipment to manage possible spikes in cases.
3. That outbreak risks are minimized in high-vulnerability settings – particularly in elderly homes, mental health facilities and for people residing in crowded places.
Again, note that the gating criteria do not address this particular concern. Rather those concerns are addressed in phases one, two and three of the program. The result is that inevitably the vulnerability of certain settings will be rationalized away by those eager to get to the gating criteria rather than urgently addressing high-vulnerability settings as a first step.
4. That workplace preventive measures are established—with physical distancing, handwashing facilities, and respiratory etiquette in place.
Enforcing safety measures in private settings will be a challenge. We are very skeptical that employers, when faced with the increased costs of implementing safety measures, will comply with them, particularly where marginalized populations (including the undocumented) are concerned. Moreover, the gating criteria simply do not address this problem at the outset, rather leaving it for later in the process.
5. That importation risks can be managed.
The gating criteria say nothing about importation risks with respect to international, interstate, or intrastate importation.
6. That communities have a voice and are engaged in the transition.
In our federalism, the states as primary actors may or may not take the voices in their communities into account. Medicaid expansion under the Affordable Care Act is the most recent example of this failure to take into account multiple voices, and that experience appears to demonstrate the improbability at local, state, and federal levels of sufficient attention being paid to the interests of all the communities that will be engaged in the transition. We wish we were not such pessimists, but having seen how the American polity operates, we are hesitant to have confidence. Take for one example, Flint, Michigan.
Taking all of these items together, the fear is that at the end of the day, there will be more dead and dying and these mechanisms for rationalizing indifference to that dying will be invoked as “neutral” criteria that lead the re-opening. This type of rationalization is an old process in American politics where the form is respected and the substance is minimized. The argument will be focused on the intent of the guidelines and not on their effect because we tend not to like having governmental action looked at for its effect.
So we fear for our fellow Americans and all residents, documented or undocumented, if this policy is followed. We fear there will be much more death and too much rationalization of that death. Especially if it is primarily among the elderly, the poor, the black and the brown.
We worry about the treatment of people like commodities in this response to the COVID-19 pandemic.
What is going on with these guidelines is nothing more or less than setting up a blame-shifting device if things go wrong. Propose guidelines. Have experts approve them. When things go wrong, blame the guidelines. Or blame the state and local authorities for not collecting the data needed to make the guidelines work.
What a people-first procedure would do is create a generous margin of error to absorb risks. It is not clear that that has been done here. There is, in essence, an acceptable level of loss among certain classes who are measured (and less concern about other classes for which measurement is more problematic). We do not have a problem with measurement in the abstract, which must be done—but with the parameters set and the resources for implementation.
It is not clear what the hospital category has to say about ventilator availability as a function of acute cases: one would have thought this to have been a clear metric of importance given all the attention paid to this by governors. Is that idea of a cushion in equipment part of the hospital column when one drills down?
We may be looking at this in a rush, but would a proper metric not include some ratio or cushion for essential supplies on hand in the area to address a spike that occurs later (some metric that measures masks, gloves, ventilators, beds, a healthy doctor/patient and nurse/patient ratio)?
Of course, while ideologically unpleasant for some, the alternative approach for the COVID-19 pandemic vulnerable could be expanded governmental support until the health crisis is clearly overcome. That cost would no doubt be significant, but arguably a relatively small price to pay as compared to the costs of a premature reopening of the economy. The important point is to understand that such an approach would not be one that denounced capitalism but would rather be one that separates capitalism from one or another ideology of capitalism (e.g., Thomas Piketty, Capitalism and Ideology) and its effects. There are many ways to channel capitalism in a health crisis. Just like during the Great Depression, capitalism had to adjust in light of dramatic unemployment. We face at least that kind of danger today and solutions like these guidelines that mask the underlying health crisis are not going to get us out of this horrible mess.
Benjamin G. Davis is a Professor of Law at the University of Toledo College of Law specializing in International Law and Alternative Dispute Resolution. He contributes to JURIST and the SALTLAW Blog.
William H. Widen is a Professor of Law at the University of Miami School of Law specializing in Contracts, Commercial Law and other business law subjects. He practiced business law for 17 years in New York City prior to joining the legal academy.
Suggested citation: Benjamin G. Davis and William H. Widen, No Market Solution for Black Death: COVID-19 Guidelines As Crime, JURIST – Academic Commentary, April 18, 2020, https://www.jurist.org/commentary/2020/04/davis-widen-covid-19-guidelines-as-crime/
This article was prepared for publication by Megan McKee, JURIST’s Executive Director. Please direct any questions or comments to her at commentary@jurist.org
